Bronchial Artery Embolisation (Bae)
Massive haemoptysis is a frightening and potentially life-threatening clinical event. Patients with chronic inflammatory lung diseases such as Tuberculosis (TB) develop markedly hypertrophied and fragile bronchial arteries that may lead to clinically significant haemoptysis. Surgical intervention is hazardous and often impossible in these patients with diffuse parenchymal lung disease. The development of bronchial artery embolization techniques has revolutionized the approach to these patients. Super-selective catheterization of the bronchial arteries feeding the affected areas followed by particulate embolization has proven to be an effective treatment for the control of bleeding. With modern microcatheters and guidewires, bronchial artery embolization is safe and well tolerated by patients. Persistent haemoptysis can be successfully controlled in as many as 90% of patients. Recurrent haemoptysis also can be successfully controlled with embolization. Therefore, despite a prior history of bleeding and prior embolization procedures, no patient should be denied the opportunity for additional transcatheter therapy.
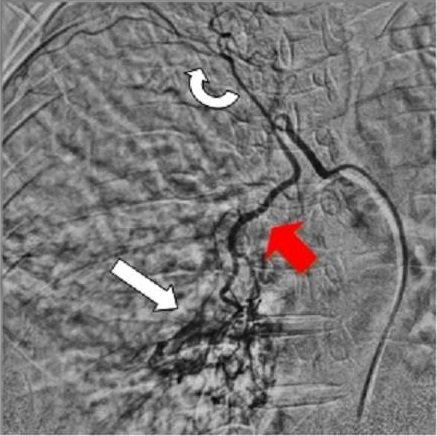
Common bronchial-intercostal trunk. Both the right bronchial artery and superior intercostal artery arise from a common trunk. The bronchial artery (straight red arrow) follows the course of the mainstem bronchus, whereas the intercostal artery follows the undersurface of the rib (curved arrow). Abnormal vessels & blush (Straight white arrow).
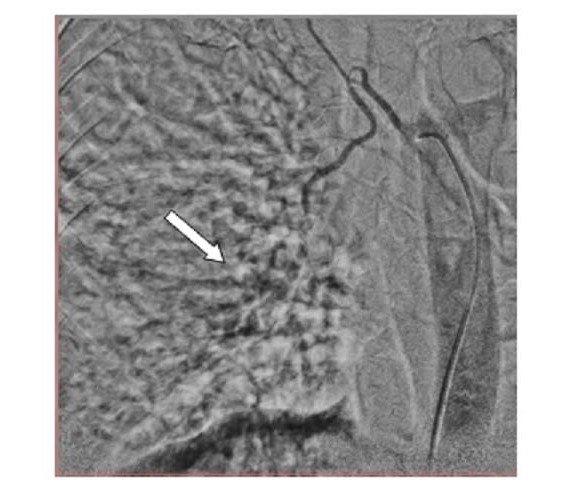
Post embolisation abnormal vessels & blush disappeared
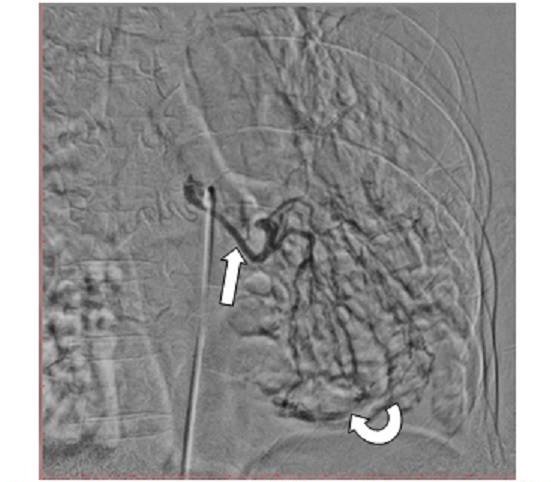
The Left bronchial artery (straight arrow) follows the course of the mainstem bronchus. Abnormal vessels & blush (Curved white arrow).
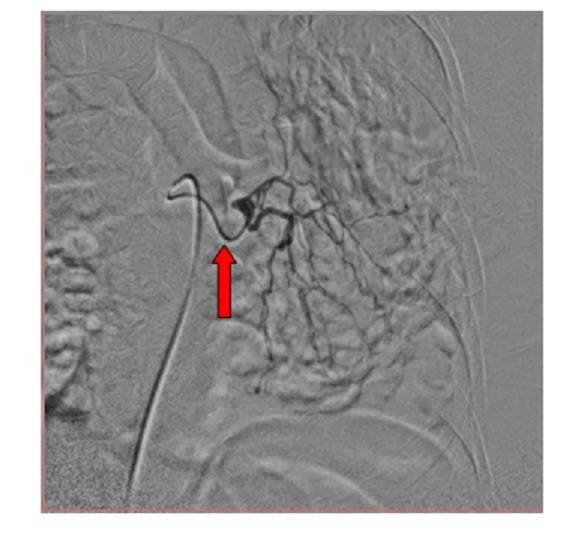
Microcatheter

Post embolisation abnormal vessels & blush disappeared